EMOTIONAL MEMORY
7.3
Emotional memory as a treatment target
Current treatment options are far from satisfactory. How could new approaches help to reduce fear symptoms? Read this article by Dominique de Quervain.
The current options for treating PTSD and phobias are mainly psychotherapy and/or anxiety-reducing and antidepressant medications. Psychotherapeutic interventions (e.g. exposure treatment) have had some success, especially in phobias, but not all patients respond sufficiently to the treatment, and the return of fear in treated patients is a well-known problem. Pharmacological first-line treatments include drugs with anxiolytic actions (e.g. benzodiazepines) for short-term use and drugs with antidepressant actions (e.g. serotonin reuptake inhibitors and other monoamine reuptake inhibitors) for long-term use. However, many patients treated with such anxiolytic or antidepressant drugs continue to have symptoms. It should be noted that such pharmacotherapies are primarily aimed at alleviating chronic stress and anxiety symptoms and fail to tackle the underlying aversive memory trace. This means that new approaches are needed.
The idea of targeting memory processes relevant to fear-related disorders has received a great deal of attention in recent years. This idea is further bolstered by evidence from neuroimaging studies that indicate a large overlap between the neural substrates of fear-related disorders and those of emotional memory processes.
Novel approaches: one proposed strategy to target memory processes to prevent PTSD is to pharmacologically reduce the initial memory consolidation of aversive events, for example by using opioids or beta-adrenergic receptor blockers. In established fear-related disorders, a different approach could be to reduce the excessive retrieval of aversive memories, thereby reducing the severity and/or frequency of symptoms such as intrusions and nightmares. A third approach would be to aid the extinction of the traumatic memory trace (a process that is often impaired in patients with fear-related disorders). A promising novel strategy to achieve this is combining drug treatment (e.g. the partial glutamate agonist D-cycloserine) with exposure therapy in a timed manner to enhance extinction and improve the long-term outcome of exposure therapy. A fourth strategy is to use pharmacological agents, such as beta-adrenergic receptor blockers, when the aversive memory trace is reactivated so as to interfere with the reconsolidation of the traumatic memory.
Our research group argues that glucocorticoid-related interventions are of special interest in the clinical context because, unlike most other memory-modifying drugs, they affect distinct memory processes that can synergistically contribute to a reduction of fear-related symptoms, i.e., by both reducing aversive memory retrieval and enhancing fear extinction. Enhancing fear extinction is of particular interest when combined with exposure therapy (see Figure 1).
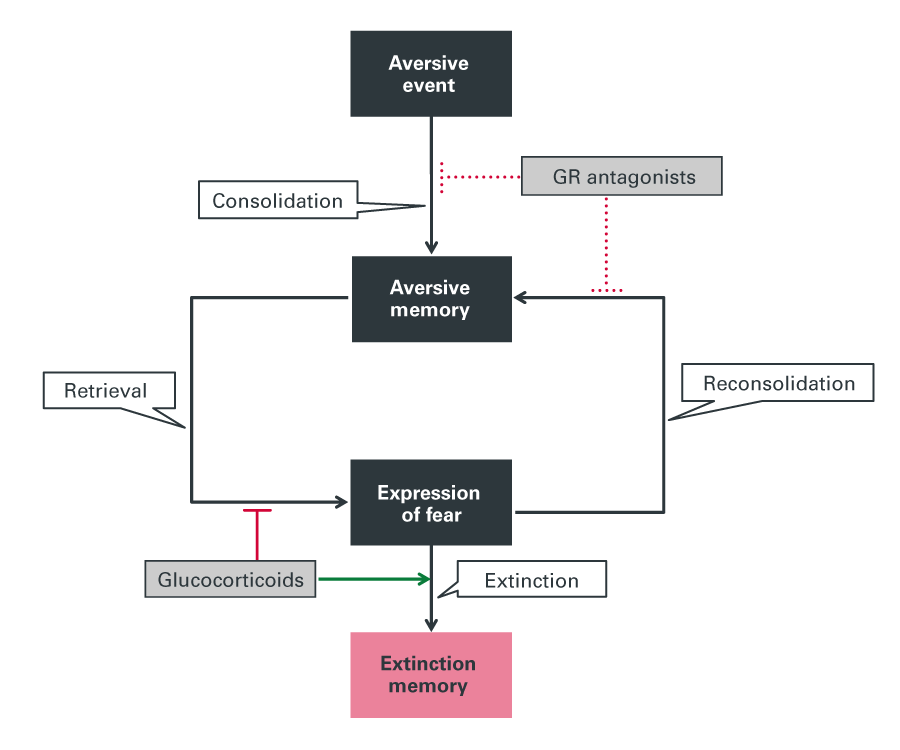
Figure 1: Glucocorticoid signaling-based intervention strategies. Glucocorticoids have been found to reduce the retrieval of aversive memory and enhance memory extinction processes. The vast majority of studies using glucocorticoids in fear-related disorder have shown a reduction of fear symptoms. At present, there are only a few studies that examine the approach of using glucocorticoid receptor (GR) antagonists to block initial consolidation of aversive memory or to block reconsolidation. Copyright: Figure adapted from de Quervain et al., Nature Reviews Neuroscience, 2017; 18(1):7-19. doi: 10.1038/nrn.2016.155.
Lizenz
University of Basel